
Juvenile Rheumatoid Arthritis
What is Juvenile Rheumatoid Arthritis?
Juvenile rheumatoid arthritis (JRA) is an inflammatory form of arthritis that affects children, usually before the age of 16. Inflammation in a joint is the defining characteristic of most forms of arthritis. JRA involves inflammation and stiffness in a joint that lasts for more than six weeks. The joint may be red, swollen and sore, although the child may not complain of joint pain.
JRA is the most common form of juvenile arthritis. It may affect one joint or many joints. Like the rheumatoid arthritis that affects adults, JRA is a systemic disease and may also affect other systems in the body. Other than the joints, the eyes are the most common area affected. Some forms of JRA may also affect the skin and other organs such as the heart, lungs, liver and spleen.
JRA affects between 30,000 and 50,000 children in the United States, according to the Arthritis Foundation. It usually does not develop in infancy but can develop any other time in childhood. Certain types more commonly develop among 6- to 8-year-olds, whereas others occur in teenagers.
Juvenile rheumatoid arthritis affects the joints, where two or more bones meet. There are several types of joints. Arthritis occurs mostly in synovial joints, which can move, such as those in the hands, wrists, ankles, knees and feet. For each synovial joint, a space enclosed by the ligaments and adjoining bones forms a cavity called the joint capsule. The outer layer of the capsule is formed by a fibrous membrane.
The inside of the capsule is lined with a membrane called the synovium. This membrane secretes synovial fluid, which fills the joint capsule and provides lubrication. The ends of the bones encased in the capsule are cushioned in soft cartilage. The cartilage and synovial fluid permit the bones to move without rubbing against each other.
JRA is an autoimmune condition, which means people with JRA have an abnormal immune response. Normally, the immune system protects the body from outside invaders, such as germs. Immune cells, such as white blood cells, attack these invaders and flush them out or make them inactive. Part of this process normally produces some inflammation in tissue.
For someone with autoimmune response, the immune system misidentifies normal body tissue as an outside invader. It attacks the tissue and tries to destroy it. In JRA, certain types of white blood cells attack parts of the synovium, causing the inflammation that characterizes JRA. The synovium then thickens, which causes the joint to swell. The synovium can form a body called a pannus, which has granular tissue that covers the bone and cartilage. The pannus tissue reacts with proteins called enzymes and erodes the bone surface.
The specific cause of JRA is not well understood. Although the immune system attacks the tissue in the joints, no one knows what triggers such an attack. Some researchers think that a genetic component is involved that makes a child more susceptible to developing JRA, but that some outside factor (e.g., viral infection) or a combination of factors trigger the initial inflammation.
JRA develops in several forms, which may affect a few joints in the body or many joints.
Joints commonly affected by JRA include:
- Lower spine
- Jaw
- Hips, knees and ankles
- Shoulders, elbows, wrists and hands
- Neck
All forms of arthritis may cause joint pain and swelling. Such joint changes in JRA may affect the growth and proper development of bones in children.
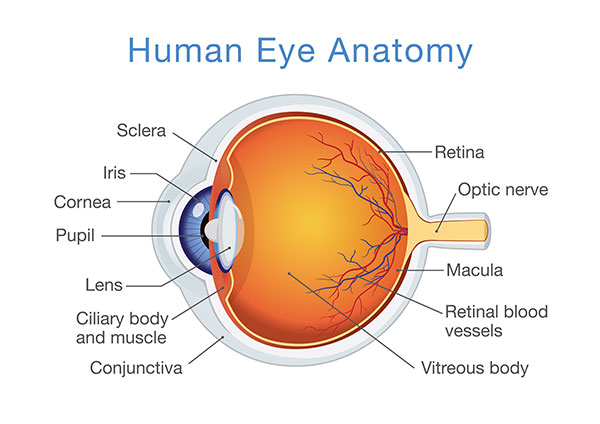
Many children with JRA also experience inflammations in the eye. Some of the inflammations involve the uveal tract, the middle layer of the eye that includes the iris, ciliary body and choroid. Some of these inflammations may not have symptoms but can cause vision problems if left untreated. Some children also develop recurrent rashes. The most severe cases of JRA can affect the heart, lungs, spleen, liver and lymph nodes.
The course of JRA may vary. Some children may have mild joint pain for a few months or a year. For others, the symptoms are recurrent over years and may affect their activity levels and result in frequent absences from school. Children may be reluctant to exercise or participate in activities because of pain.
Most children eventually outgrow JRA and are not affected by it as adults. Some patients may experience joint problems as adults, especially if their bones were affected during a growth period. According to the National Institutes of Health, about 75 percent of children with JRA enter remission eventually with a minimal loss of function and deformity. Other cases of JRA may actually be the adult form of rheumatoid arthritis that began at an early age.
Types and differences of JRA
Juvenile rheumatoid arthritis (JRA) is divided into three categories, which are characterized by the number of joints and other body systems affected. These categories are:
Pauciarticular JRA
This form involves four or fewer joints. It is the most common form of JRA and affects half of the children with the disease, according to the National Institutes of Health (NIH). Pauciarticular JRA usually involves the larger joints, such as the knee, ankle, wrist or shoulder. It usually occurs asymmetrically, affecting a joint on only one side of the body (e.g., one knee). Children with pauciarticular JRA frequently have eye inflammations.
Polyarticular JRA
This form affects five or more joints and is more common in girls than boys. It involves the small joints in the fingers and hands, and usually occurs symmetrically, in the same joints on both sides of the body. The knees and hips are also commonly affected. Some children may have jaw pain, which can cause discomfort when chewing and may affect eating habits. Polyarticular JRA is more severe and may also include eye inflammations. It affects about 30 percent of children with JRA, according to the NIH. Some children with polyarticular JRA actually have adult rheumatoid arthritis that develops at an early age.
Systemic JRA
This form of JRA is also known as Still’s disease. Systemic JRA affects about 20 percent of the children with JRA, according to the NIH. It can affect many body systems and have other symptoms, such as fever and rash, that may appear several months before any joint pain. Systemic JRA can cause inflammation of the heart (pericarditis) and lungs (pleuritis) and can enlarge the liver, spleen or lymph nodes. Flare-ups may occur after a child has a viral infection, such as chicken pox. Systemic symptoms may disappear in adulthood, but the arthritis may persist. The development of systemic JRA later in life is known as adult-onset Still’s disease.
Signs and symptoms of JRA
The symptoms of juvenile rheumatoid arthritis (JRA) may take several weeks or months before they are noticeable. Children may experience joint pain or swelling but might not complain about it. Some may have stiffness, especially early in the morning or after a nap. A child with an affected knee may limp in the morning but get better later in the day.
The signs and symptoms may vary from day to day, or even within one day. Certain eye problems associated with JRA may have no symptoms.
The most common symptoms associated with JRA include:
- Joint pain, swelling or stiffness. A joint must be swollen for at least six weeks to be considered for a diagnosis of JRA.
- Muscle aches. Usually affect muscles throughout the body, and not just one part.
- Fever. High fevers that come and go occur with systemic JRA. Low-grade fevers are common with polyarticular JRA.
- Skin rash. A pink rash occurs with systemic JRA.
- Rheumatoid nodules. Painless lumps under the skin at the elbows and feet may be found in some children with polyarticular JRA.
- Eye problems. Redness, eye pain and sensitivity to light may occur in children with some forms of polyarticular JRA.
- Swollen lymph nodes. These may occur in children with systemic JRA.
Some children do not complain of pain, but parents or others may notice other signs of illness.
Some JRA signs parents may notice include:
- Limping or other gait disturbances, especially in the morning. This can be an early sign due to involvement of a knee joint.
- Reluctance to use an arm or leg.
- Reduced activity level.
- Changed dental or eating habits as a result of jaw pain, dental pain or orofacial pain.
Diagnosis methods for JRA
Juvenile rheumatoid arthritis (JRA) may be difficult to diagnose. Many children may not experience identifiable symptoms, or the symptoms they do have may be caused by other conditions, such as systemic lupus erythematosus, Lyme disease or bone disorders.
The first sign is usually a complain of joint pain or swelling by the child, or sometimes a limp noticed by parents. A diagnostic visit for JRA can be conducted by a child’s pediatrician. A pediatrician who suspects JRA may refer the case to a pediatric rheumatologist, a physician who specializes in arthritis and other inflammatory diseases in children.
A physical examination includes checking the joints for swelling, warmth, tenderness and range of motion. The physician notes descriptions and incidences of pain and its duration. The physician may try to move various joints to see if motion causes pain. The diagnosis will also include a medical history, including any family history of arthritis or autoimmune conditions, previous injuries or surgeries and general use of the joints. The physician will also note any fevers, rashes or infections.
Many laboratory tests are used to screen for specific kinds of arthritis or other diseases. Certain blood tests may produce characteristic results for some types of JRA, and thus may be used to classify which type of JRA is present. None of these tests definitively diagnose JRA.
Some of the blood tests include:
Complete blood count (CBC)
Measures the levels of different types of blood cells. Children with JRA may show a low count of red blood cells (anemia) and higher counts of white blood cells.
Erythrocyte sedimentation rate (ESR, or sed rate)
If elevated, indicates inflammation, which may be related to many causes of inflammation or infection. It is always elevated for systemic and polyarticular JRA but may be within the normal range for children with pauciarticular JRA.
Antinuclear antibody (ANA) test
Tests for certain autoimmune disorders such as lupus. Not all children with JRA have this antibody. Those who test positive for ANA are more likely to develop eye inflammations such as uveitis. Children with systemic JRA usually test negative for ANA. This antibody is found positive in 75 to 85 percent of cases of pauciarticular JRA, 40 to 50 percent of cases of polyarticular JRA and about 10 percent of cases of systemic JRA.
Rheumatoid factor test
Identifies the presence of the rheumatoid factor (RF) antibody. Children with systemic JRA usually test negative for rheumatoid factor. Some children with polyarticular JRA test positive for RF. RF testing thus helps differentiate among the three types of JRA.
Another test that may be used for JRA is a synovial fluid analysis. Fluid from an affected joint is withdrawn with a needle (a procedure called arthrocentesis). Examining this fluid may help determine if the inflammation is caused by JRA or some other condition. Arthrocentesis is also used to diagnose any joint infection.
A diagnostic examination where JRA is suspected may also include x-rays. Images are taken of the affected joints and may help rule out other potential causes. Additional tests may also be used to rule out other potential bone problems, such as congenital deformities or bone cancer. These include CAT scans (computed axial tomography), where multiple x-ray images are taken, and MRI (magnetic resonance imaging), which uses powerful magnets to form an image of the bone and tissues.
When JRA is suspected, a pediatrician will also refer the patient to an ophthalmologist, a physician who specializes in eye diseases. Children with JRA are susceptible to eye inflammations, which may not exhibit symptoms. The ophthalmologist may perform an examination with a device called a slit lamp, which has high-intensity light that can be focused in a narrow area. It is used to examine some of the structures of the eye such as the iris and other parts of the uveal tract (middle eye) that are subject to inflammation. Children with JRA should receive eye examinations by an ophthalmologist at least every six months.
Treatment and prevention of JRA
Juvenile rheumatoid arthritis (JRA) cannot be cured, although many children outgrow the symptoms. Some children have mild symptoms for a few years. The goal of treatment is to maintain a high level of physical and social functioning. For others, JRA affects and deforms the joints, causing pain and interfering with growth. Most treatment plans for JRA involve regular monitoring of children and medications to ease their joint pain.
Exercise can be a regular part of a child’s treatment for JRA. Exercise helps to develop strong muscles and bones, keeps joints flexible and helps to build endurance. Some children may need physical therapy, occupational therapy or both to learn how to recover any lost range of motion, protect their joints and adapt to daily tasks. The therapist may recommend ways to maintain a child’s normal bone growth, such as splints or joint-protection techniques.
Treatment plans that educate family members and the child’s school community about JRA and its effects can also prove beneficial. Joining a support group and explaining the disease to the child are helpful in coping with this chronic illness.
Regular monitoring of JRA and its effects on other systems is essential. Children with JRA require eye examinations by an ophthalmologist at least every six months.
The most common treatments for JRA are medications. A range of prescription and nonprescription medications are used to alleviate the pain and inflammation. Some of the medications used to treat JRA include:
Nonsteroidal anti-inflammatory drugs (NSAIDs)
These drugs are used to reduce pain and inflammation. They are considered the first line of treatment for all forms of JRA. Most children with pauciarticular JRA and some with polyarticular JRA respond to NSAIDs without additional drugs. Nonsteroidal anti-inflammatory drugs come in prescription and nonprescription forms. Some may affect kidney or gastrointestinal function. Aspirin is generally not recommended for children because of the risk of Reye’s syndrome, a rare but potentially fatal condition that affects organs through the body.
Disease-modifying antirheumatic drugs (DMARDs)
This category includes many types of drugs that suppress the overactive immune response of JRA. They are a second line of treatment, after NSAIDs. Disease-modifying antirheumatic drugs work long term and can take several months to produce results. All DMARDs have some side effects, including gastrointestinal problems, some serious liver or kidney complications and repressed immune responses to infection.
Biologic response modifiers (BRMs)
Drugs that slow progression of the disease and inhibit the production of the proteins called cytokines, which contribute to inflammation. BRMs block proteins that cause inflammation, such as tumor necrosis factor (TNF) or interleukin-1. These drugs may be prescribed for children with polyarticular JRA who have not experienced relief from other treatments.
Corticosteroids
May be given as pills or injections. For serious cases of JRA, corticosteroids may be used to stop systemic symptoms such as pericarditis (inflammation of the heart sac). Corticosteroids may interfere with a child’s growth, weaken bones and increase susceptibility to infections. They will be prescribed at the lowest dose and for as short a time period as possible. Corticosteroids in eye drop form may be used for eye inflammation related to JRA.
All medications have some side effects, which may vary from patient to patient. Physicians monitor their patients and may adapt the medications depending on response and side effects. Sometimes complimentary or alternate therapies, such as acupuncture, can be incorporated in treatment if the physician thinks it may help the child.
Surgery is rarely used to treat JRA. Certain types of arthroplasty might be recommended in some severe cases where a joint has become damaged.
People often outgrow the symptoms of JRA, and during childhood the disease need not be debilitating. One recent study found that, unlike some other rheumatic diseases, JRA was not linked with cognitive, emotional or social problems in children.
There is no way to prevent JRA. However, early intervention and careful monitoring of children with JRA can limit the progression of the disease.
Questions for your doctor about JRA
Preparing questions in advance can help patients have more meaningful discussions with their physicians regarding their conditions. Patients or parents may wish to ask their doctor the following questions about juvenile rheumatoid arthritis (JRA):
- How do you know my child has juvenile rheumatoid arthritis (JRA) and not some other form of arthritis?
- What diagnostic tests will be used?
- What do these tests involve? Do we need to do anything to prepare for them?
- Will this condition worsen as my child gets older?
- Can the joint pain of JRA affect my child’s growth?
- Which drugs can help JRA?
- Do these drugs have side effects that are harmful for a child?
- Can other treatments or therapies help?
- Should I watch for symptoms in body areas or systems other than the joints?
- Will exercise or sports participation help or hurt my child’s JRA?
- How can we tell when it’s best to be active and when it’s best to rest?
Additional Information
Medications
Activity
- During an attack, keep the child in bed, except to use the bathroom, until fever and other symptoms subside.
- Splints may be necessary to support and protect an inflamed joint.
- After an attack passes, the child may gradually resume normal activities with rest periods during the day. The child should not become overtired and should sleep at least 10 to 12 hours each night.
- Physical therapy exercises will be prescribed. Some the child can do alone, and some the parents will perform for the child. It is important that the child does the exercises because they help minimize pain and the crippling effects of rheumatoid arthritis.
- Because of periodic changes in the symptoms, the physical therapy program will need revising occasionally.
- In general, contact sports should be avoided, but the child should be encouraged to participate in other school, home or community activities.
Diet
Provide a nutritious, balanced diet and encourage the child to eat.
What might complicate it?
- Involvement of tissues other than joints, producing uveitis (eye inflammation), an enlarged spleen, pericarditis or inflammation of the heart muscle.
- Permanent joint deformity.
Notify your physician if
- Your child has symptoms of juvenile rheumatoid arthritis.
- The following symptoms occur during treatment:
- Chest pain or fever.
- Appetite loss.
- New, unexplained symptoms develop. Drugs used in treatment may produce side effects.