
Rheumatoid Arthritis
What is Rheumatoid arthritis?
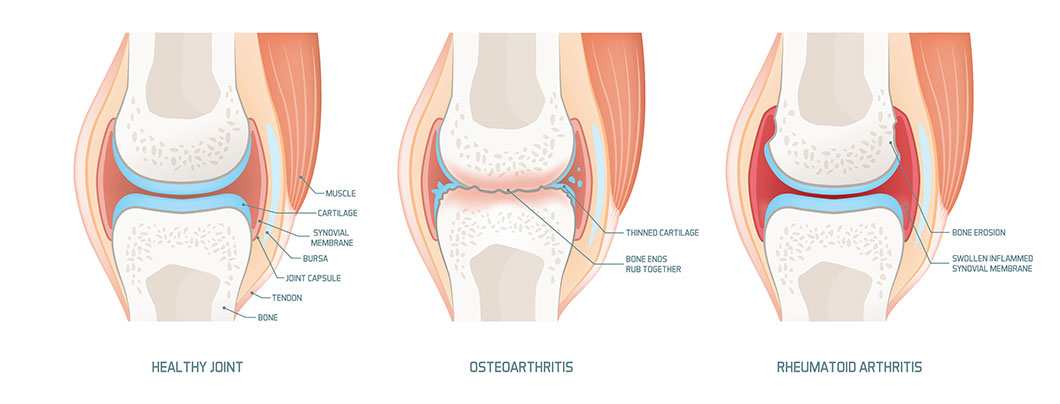
RA begins in the joints, where two or more bones meet. There are several types of joints. Arthritis occurs mostly in synovial joints, which can move, such as those in the hands, wrists, ankles, knees and feet. For each synovial joint, a space enclosed by the ligaments and adjoining bones forms a cavity called the joint capsule. The outer layer of the capsule is formed by a fibrous membrane. The inside of the capsule is lined with a membrane called the synovium. This membrane secretes synovial fluid, which fills the joint capsule and provides lubrication. The ends of the bones encased in the capsule are cushioned in soft cartilage. The cartilage and synovial fluid permit the bones to move without rubbing against each other.
People with RA experience inflammation in the joint capsules, which affects the movement of the joint and causes pain. RA is an autoimmune condition, which means people with RA have an abnormal immune response. Normally, the immune system protects the body from outside invaders, such as germs. Immune cells (e.g., white blood cells) attack these invaders and flush them out or make them inactive. Part of this process normally produces some inflammation in tissue.
For someone with autoimmune response, the immune system misidentifies regular body tissue as an outside invader. It attacks the tissue and tries to destroy it. In RA, certain types of white blood cells attack parts of the synovium, causing the inflammation that characterizes RA. The process by which this occurs is not well understood. The synovium thickens, which causes the joint to swell. The synovium can form a body called a pannus, which has granular tissue that covers the bone and cartilage. The pannus tissue reacts with enzymes and erodes the bone surface.
RA usually begins in the smaller joints of the fingers or feet. It frequently occurs in the same joints on both sides of the body. It eventually may move to involve more joints, including the wrists, ankles, elbows and knees.
RA is a chronic condition, but attacks may vary. There are periods of severe inflammation called flare-ups, and RA can go into remission for long periods of time. A few people may experience one flare-up followed by remission. However, RA is generally a progressive (worsening) illness. It may start in a few small joints and eventually spread to other joints and tissues, such as cartilage, bones and ligaments. Some RA patients eventually have substantial functional disability that prevents them from working.
RA is a systemic disease, meaning it can involve other body systems. RA can affect the linings of the heart, lungs and blood vessels. It can also affect the eyes and the nerves. Inflammation of the blood vessels (vasculitis) can be life-threatening, causing skin ulcerations and infections, bleeding ulcers, hemorrhage and nerve problems.
Rheumatologists classify the status of RA patients based on their ability to function:
- Class I. Completely able to perform usual activities of daily living.
- Class II. Able to perform usual self-care and work activities, but limited in other activities (i.e., sports or chores).
- Class III. Able to perform self-care activities but limited in work and other activities.
- Class IV. Limited in ability to perform usual self-care, work and other activities.
RA can occur at any age and in all races and ethnic groups. It generally begins between the ages of 30 and 50. Although adults are primarily affected, the condition can affect children as well. For more information, see Juvenile Rheumatoid Arthritis.
Women are more commonly affected by RA than men. Of the 2.1 million Americans with RA, 1.5 million are women, according to the National Institutes of Health (NIH). Women with RA tend to experience remission of symptoms during pregnancy and flare-ups after giving birth or while breastfeeding. The NIH notes that the number of RA cases appears to be decreasing for unknown reasons.
RA is not the same as osteoarthritis (OA), the degenerative form of arthritis most common among elderly people. Although both forms of arthritis cause joint pain, there are several major differences:
- OA involves degeneration of joint cartilage. RA involves inflammation of the membranes lining joints.
- RA usually occurs symmetrically, such as in both hands or both knees. OA may occur on one side (e.g., in one knee).
- OA affects only the joints. RA can affect other systems in the body, including the lungs, nerves or heart.
Risk factors and causes of rheumatoid arthritis
The specific cause of rheumatoid arthritis (RA) is unknown. Although the immune system attacks the tissue in the joints, no one knows what triggers such an autoimmune attack, or why it first attacks only a few joints. Some researchers think that some outside factor or a combination of factors trigger the initial inflammation.
Risk factors are elements that may increase a person’s likelihood of developing a disease or condition. For RA, risk factors may be divided into two groups. Susceptibility factors may indicate a person is susceptible to the disease. Initiating factors are those that may occur with the susceptibility factor and trigger RA. The presence of a risk factor does not mean a person will develop the condition, and the absence of a risk factor does not mean the condition will not occur.
Some of the susceptibility risk factors for RA include:
- Sex. RA is much more common in women. Women make up about 70 percent of the RA cases in the United States, according to the Arthritis Foundation (AF).
- Age. RA can occur at any age but usually begins between the ages of 30 and 50.
- Family history and genetics. Having immediate family members with RA (parents, siblings or children) increases the likelihood of developing the disease. One of the genes associated with RA is HLA-DR4. This gene is present in some percentage of the entire population, but they may not develop RA. However, about two-thirds of Caucasian RA patients have this gene, according to the AF. Presence of another autoimmune disease. People with an autoimmune disorder, such as Sjogren's syndrome, type 1 diabetes or lupus, are at greater risk for developing others.
Some of the known or suspected initiating risk factors for RA include:
- Smoking. People who smoke have a higher risk of developing RA. Smoking may also be a factor that initiates inflammation.
- Infection. A previous infection with bacteria or a virus may help initiate RA. The link is suspected, but there is no evidence yet to support it.
- Lifestyle factors. Stress and diet may also be factors that can initiate RA inflammation, but no studies have proven this as of yet.
Signs and symptoms of rheumatoid arthritis
The symptoms of rheumatoid arthritis (RA) begin gradually. It may be weeks or months before they are noticeable. Many people experience nonspecific symptoms, such as fatigue, malaise, loss of appetite and low-grade fevers. The joint symptoms begin with morning stiffness that may last an hour or more. Joint pain, stiffness and swelling that occurs symmetrically (same joint on both sides of the body) are also characteristic of RA.
Some people develop rheumatoid nodules, which are painless lumps under the skin that form at pressure points, such as feet, hands and elbows. Dry eyes and mouth, which are part of a separate condition known as Sjogren's syndrome, are also characteristic of RA.
RA causes some particular symptoms in each of the joints it affects. Some of the symptoms in specific joints include:
Hand
Joints in the fingers and hands are usually the first joints affected by RA. They may become red, swollen and tender. Nodules may form that restrict hand movement. Gripping may become more difficult and the thumb may lose mobility. As RA progresses, characteristic problems include the tightening of the tendon on the back of the hand so it becomes prominent and deformities where the fingers shift toward the little finger (ulnar drift).
Wrist
In early RA, the wrist may not bend back easily. In later stages, inflammation to the joints and tendons in the wrist can make the tendons rupture. Pressure on the median nerve in the wrist may cause carpal tunnel syndrome, a painful wrist condition.
Elbow
Inflammation and swelling at the elbow can compress nerves and cause numbness or tingling in the fingers.
Shoulder
In later stages of RA, some inflammation may limit motion and cause shoulder pain, including the condition known as frozen shoulder.
Foot
The joints in the feet are also among the first affected by RA. There may be tenderness and pain in the joint at the base of the big toe, which may form a bunion. Redness, swelling and heel pain may also occur.
Ankle
Inflammation in the ankle joint may compress nerves and cause numbness or tingling in the feet.
Knees
RA may make it difficult to bend the knee and cause swelling. A fluid-filled sac called a Baker’s cyst may form at the back of the knee. Progression of RA degenerates cartilage and weakens the ligaments. This may create the sensation of knee instability.
Hips
Later stages of RA may inflame the hips, making it painful to walk.
Neck (cervical spine)
Most people with RA in the neck have had the disease for 10 years or more. Inflammation can cause a stiff neck and inability to bend or turn the head. Later inflammation in the neck can cause serious pressure on the spinal cord, which may result in arm pain, loss of coordination and loss of bowel and bladder function.
Windpipe
Nearly one-third of people with RA have inflammation of the cricoarytenoid joint in the neck near the windpipe (trachea), which can cause difficulty breathing and hoarseness.
If RA moves to other body systems, it may cause the following symptoms:
- Lungs. Inflammation of the lung lining may cause chest pain with deep breathing or coughing.
- Cardiovascular system. Nearly all RA patients have anemia, a lowered level of red blood cells, which can cause fatigue. RA in the heart may cause chest pain when leaning forward or lying down, although this is rare. Inflammation in blood vessels (vasculitis) can slow blood supply to tissues. This may produce symptoms in different locations, depending on the affected blood vessels. It may first be visible as leg ulcers and black areas around the nail beds.
- Nervous system. RA in any part of the nervous system may cause numbness, weakness or tingling.
Diagnosis methods for rheumatoid arthritis
Diagnosis of rheumatoid arthritis (RA) includes a combination of detailed medical history, physical examination, laboratory tests and imaging studies. Patients may be asked to complete a pain assessment form. There is not one specific test that can definitively diagnose the disease.
During the physical examination, the joints will be checked for swelling, warmth, tenderness and range of motion. The physician notes descriptions and incidences of pain and its duration. The physician may try to move various joints to see if motion causes pain. The diagnosis will also include a medical history, including any family history of arthritis or autoimmune conditions, previous injuries or surgeries and general use of the joints, including stiffness in the morning lasting more than one hour.
RA may be difficult to distinguish from other arthritic disorders. A primary care physician who suspects or diagnoses RA may refer may refer the patient to a rheumatologist, a physician who specializes in arthritis and other diseases of the muscles, joints and bones. Several other conditions may have symptoms similar to RA and must be ruled out. These conditions include other forms of arthritis and systemic lupus erythematosus.
Many laboratory tests are used to screen for specific kinds of arthritis or other diseases. Certain blood tests frequently produce characteristic results in RA patients, but do not definitively diagnose RA.
Some of these blood tests include:
- Complete blood count (CBC). This routine blood test measures the levels of different types of blood cells. People with RA may show a low count of red blood cells (anemia) and higher counts of white blood cells and platelets.
- Erythrocyte sedimentation rate (ESR). A high ESR indicates inflammation, which may be due to many causes.
- C reactive protein test. An elevated level of this protein produced by the liver suggests an inflammatory disease such as RA.
- Antinuclear antibody (ANA) test. Tests for certain autoimmune disorders such as RA and systemic lupus erythematosus.
- Rheumatoid factor (RF) test. Identifies the presence of the RF antibody. This may indicate RA or other autoimmune conditions such as Sjogren's syndrome, which is characterized by dry eyes and dry mouth. The test may be negative in early stages of RA or when the disease is in remission, with no flare-ups of inflammation. This antibody is usually present in 60 percent of patients in the first year of disease and in 80 percent of patients who have chronic RA.
- Cyclic citrullinated peptide antibody (CCP) test. Identifies the presence of an antibody to citrulline, an amino acid. This test may identify RA at an earlier stage than the RF test. The CCP test may be ordered along with the RF test, or after a patient with symptoms has tested negative for RF.
Another test commonly used for RA is a synovial fluid analysis. Fluid from an affected joint is withdrawn with a needle (a procedure called arthrocentesis). In addition to RA, the fluid may indicate gout, infectious arthritis or juvenile rheumatoid arthritis.
A diagnostic examination where RA is suspected may also include x-rays.However, when RA is in its early stages, x-rays may not show much disease. X-rays are useful to differentiate RA from osteoarthritis, which is much more apparent in early x-rays. Images taken in early stage RA can serve as a baseline to monitor the changes in the joints. MRI (magnetic resonance imaging) and ultrasound provide better views of the soft tissues but are not commonly used. Ultrasounds may be useful for RA in the hands.
The American College of Rheumatology has established criteria for clinical classification of RA:
- Morning joint stiffness for more than one hour.
- Swelling of three or more joint areas simultaneously.
- Swelling in the wrist or two of the three finger joints.
- Swelling of the same joints on both sides of the body.
- Rheumatoid nodules.
- Positive blood test for rheumatoid factor.
- X-ray changes that include erosions or decalcification of bones near joints.
Patients can be classified as having RA if they have four or more of the criteria listed. The first four listed must have been present for at least six weeks.
Treatment and prevention of rheumatoid arthritis
There is no known cure for rheumatoid arthritis (RA). For a few people, the disease has mild symptoms that never get worse. For others, it progressively affects and deforms the joints, causing pain and reducing mobility.
Once diagnosed, RA usually requires lifelong treatment and monitoring. Treatment begins with educating the patient about the disease and risk of joint damage and loss of function. No single treatment plan is effective for all RA patients. Initial treatment may concentrate on alleviating pain, preventing loss of function and slowing the degeneration of joints. Early, aggressive medical treatment can slow the progress of the disease.
Regular monitoring of RA and its effects on other systems is essential. RA patients should have their condition assessed at regular physical examinations every six months.
RA patients are more likely to develop certain other medical conditions, including coronary artery disease and osteoporosis. Adequate nutrition and attention to diet may minimize this likelihood.
Exercise and loss of excess weight may help RA by relieving excess strain on the joints and maintaining muscle tone around the joints. People with RA should consult their physician before beginning or changing any weight loss or exercise program. A home exercise regime may be part of a physical therapy program that addresses strength, range of motion, flexibility and endurance. Occupational therapy may also help RA patients identify their abilities and the best ways to use their joints.
Many lifestyle factors can be adjusted for RA. Adequate amounts of sleep and resting when experiencing fatigue are important. The National Institutes of Health recommends that RA patients account for their flare-ups and take shorter rest breaks sporadically during activity, rather than complete bed rest. Rest can reduce inflammation from RA, whereas exercise relieves stiffness.
Home life can be adjusted with special fasteners and grips for weakened hands and items such as grab bars in showers and raised toilet seats. Assistive devices that support joints can reduce the stress on them. These include braces, splints, canes, walkers, and shoes with inserts.
The chronic nature of RA and its symptom flare-ups can frustrate many patients. Relaxation methods and stress reduction techniques (e.g., yoga) may help some people cope with the disease. Biofeedback helps some patients increase control over muscle tension and certain body functions.
Some people respond to heat treatment (thermotherapy) or cold treatment (cryotherapy). A physician or physical therapist can indicate which kind of therapy should be used. Heat relieves pain and stiffness. Cold relieves pain and may reduce swelling. Either may incorporate water therapy (hydrotherapy). People with some medical conditions, such as poor circulation, should not use cryotherapy, and conditions such as impaired sensation may rule out thermotherapy.
Some patients may consider complementary and alternative therapies to relieve pain associated with RA. For example, many people take the nutritional supplements glucosamine and chondroitin for arthritis pain relief and to strengthen cartilage. Studies have found that these two supplements may be helpful with some cases of osteoarthritis, but scientific evidence of their usefulness with RA is lacking.
Topical treatments and supplements may also alleviate RA pain. Capsaicin cream has the same active substance as hot chili pepper and may lessen the pain for some patients. Patients should consult with their physician before using any alternative therapy.
RA generally responds well to early, aggressive medical intervention. A range of prescription and nonprescription medications are used to alleviate RA pain and inflammation and to slow the disease’s progress.
Some of the medications used to treat RA include:
Acetaminophen
May relieve pain associated with RA but does not affect inflammation.
Nonsteroidal anti-inflammatory drugs (NSAIDs)
NSAIDs are used to reduce pain and inflammation but do not stop RA’s progression. They come in prescription and nonprescription forms. Some may affect renal or gastrointestinal function.
Among the prescription NSAIDs are a group called COX-2 inhibitors. However, several of these drugs have potentially serious side effects, such as increased risk of heart attack, stroke and gastrointestinal bleeding. Several COX-2 inhibitors were withdrawn from sale, but others remain on the market with more specific warning labels.
Disease-modifying antirheumatic drugs (DMARDs)
This category includes many types of drugs that suppress the overactive immune response of RA and slow its progress. Prompt, aggressive use of DMARDs may be indicated for people with high rheumatoid factor (RF) levels in their blood or RA involvement in other systems.
DMARDs work long term and can take several months to produce results. All DMARDs have some side effects, including gastrointestinal problems, some serious liver or kidney complications and repressed immune responses to infection. Studies show that DMARDs alone tend to be less effective over time. Some are used in combination with NSAIDs or other drug therapies.
Biologic response modifiers (BRMs)
Drugs that slow progression of the disease and inhibit the production of the proteins called cytokines, which contribute to inflammation. BRMs block proteins that cause inflammation, such as tumor necrosis factor (TNF) or interleukin-1. Many RA patients respond favorably and achieve lengthy remissions when BRMs are combined with DMARD treatment. The BRMs known as TNF inhibitors may reduce the increased risk of cardiovascular problems in RA patients, according to recent research.
Some studies have suggested that some BRMs may increase the risk of lymphoma and other cancers, but recent data from the U.S. National Data Bank of Rheumatic Disease indicate that risk of cancer is not increased, with the exception of skin cancer.
Corticosteroids
May be given as pills or injections into the affected joint. These anti-inflammatories have some benefits for RA patients, but those may diminish in time. When corticosteroids are administered with DMARDs, they enhance the effectiveness of DMARDs. Physicians monitor corticosteroid use closely because it can cause bone loss, which is more likely for RA patients, regardless of treatment. Any bone loss can contribute to osteoporosis and fractures. Other possible complications of long-term use of corticosteroids include diabetes, glaucoma and cataracts.
Recent research suggests that combination therapy, such as taking DMARDs and a corticosteroid or taking a DMARD and a BRM, may be more effective than monotherapy. Selection of medication requires a preassessment of the prognosis. Usually prognosis is poor if there is onset of RA at early age, high titers of rheumatoid factor, elevated sedimentation rate and swelling of more than 20 joints. All medications have some side effects, which may vary from patient to patient. Physicians monitor their patients and may adapt the medications depending on response and side effects.
Another medical treatment is immunoadsorption (Prosorba column). In this process, the patient’s blood is removed through a tube and filtered through a small device that treats the antibodies from the blood and then sends the blood back to the body. The procedure is performed weekly for 12 weeks and takes two to three hours at a time.
Immunoadsorption is usually reserved for people with severe RA who have not responded to drug therapies. Studies have shown the treatment has slowed RA progress in one-third to one-half of people treated. Side effects may include an increase of RA joint pain during or after the procedure, infections related to the use of catheters, anemia, fever and a drop in blood pressure. The procedure is not recommended for patients with certain heart problems, including those taking ACE inhibitors, a class of blood pressure drugs.
Some physicians may recommend transcutaneous electrical nerve stimulation (TENS), a form of electrical therapy in which a device delivers mild electric current to the nerves to interfere with transmission of pain signals. Several studies have had conflicting results about its effect on RA pain. It has no effect on the inflammation.
Several types of surgery can correct damage to joints affected by RA. Joint surgeries range from minor procedures to total joint replacements. They are commonly performed on the knees, hands, hips and parts of the spine.
Some of the most common surgeries for RA include:
- Synovectomy. The synovial lining of a joint can be removed, either by open surgery or arthroscopy.
- Arthroscopy. A minimally invasive procedure where a lighted tube is inserted into a joint to examine tissue. Instruments attached to the tube can remove cartilage, fluid or bone fragments.
- Osteotomy. Surgery that reshapes deformed bones by removing damaged tissue and torn or loose fragments. It is most commonly performed on the knee.
- Arthrodesis. Surgery to fuse bones in a joint. It can reduce pain, but the joint will no longer move.
- Arthroplasty. Open surgery on damaged joints may also be performed to repair or replace all or part of a joint. When a joint is completely degenerated, surgeons can replace the entire joint. This is most commonly performed for the knees and hips but can also be performed in fingers, shoulders and other joints.
- Spinal surgery. Several spinal operations may be performed for RA patients, to realign the spine, ease pressure on compressed nerves or fuse the vertebrae.
In most cases, there is no known way to prevent RA. However, early intervention can limit the progression of the disease. In an analysis of data collected from 1977 to 1998, the average disability levels experienced by RA patients have declined by 40 percent, according to scientists sponsored by the National Institute of Arthritis and Musculoskeletal Diseases. The introduction of newer drug treatments since the data were compiled for that study indicates a likelihood of more disability reduction in the future.
People may be able to help prevent RA by not smoking. Scientists have found that smokers have increased risk of RA if they have antibodies against the amino acid citrulline, especially if they carry two copies of a gene called HLA-DR shared epitope (SE) genes. Recent research has also found an increased risk of RA in female smokers who have no known genetic risk factors for the disease.
Questions for your doctor regarding RA
Preparing questions in advance can help patients have more meaningful discussions with their physicians regarding their conditions. Patients may wish to ask their doctor the following questions about rheumatoid arthritis (RA):
- How do you know I have RA and not some other form of arthritis?
- Will RA spread to other joints in my body?
- What tests will confirm my condition? Will I need to take them again to monitor the disease?
- What drugs can help my condition? Do I need to take them all the time or only when I have pain?
- Should I watch for symptoms in body areas or systems other than my joints?
- Do the different types of drugs have the same effects?
- What changes should I make in my diet to help RA?
- Will exercise improve or worsen my pain?
- How do I know when I should exercise and when I should rest?
- Can physical therapy, occupational therapy, heat therapy, cold therapy, water therapy, biofeedback or other such treatments help me?
- Is it possible my RA may require surgical treatment? If so, what type of surgery is recommended, and what is the prognosis?
Additional Information
Medications
- Nonsteroidal anti-inflammatory drugs, including aspirin and other salicylates; gold compounds; immunosuppressive drugs.
- Cortisone drugs usually relieve pain dramatically for short periods, but they are less effective for long-term use. They don't prevent progressive joint destruction, and they sometimes have hazardous side effects. Cortisone injections into joints can temporarily relieve pain.
 Ibuprofen
Ibuprofen 
Activity
- Stay in bed, except to use the bathroom, until fever and other signs of an active flare-up disappear.
- Remain active, but include daily rest periods. Sleep for 10 to 12 hours each night. Don't become overtired.
- Stand, walk and sit erectly.
- When able, exercise actively to preserve strength and joint mobility. Build up slowly to the amount suggested. Exercising in a heated pool is good for stiff joints.
- Exercise disabled joints passively to help prevent contractures.
Diet
Eat a normal, well-balanced diet. Avoid arthritis diet fads, which are common. Lose weight if you are obese. Obesity stresses the joint.
Alternatives
Pseudogout, systemic lupus erythematosus, scleroderma, polyarthritis, osteoarthritis, and osteoporosis must be ruled out.
Notify your physician if
- You or a family member has symptoms of rheumatoid arthritis.
- The following occur during treatment:
- Fever or symptoms appear in previously unaffected joints.
- New, unexplained symptoms develop. Drugs in treatment may produce side effects.
- Aletaha D et al. 2010 rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum 2010 Sep; 62:2569. (http://dx.doi.org/10.1002/art.27584)