
Asthma
What is Asthma?
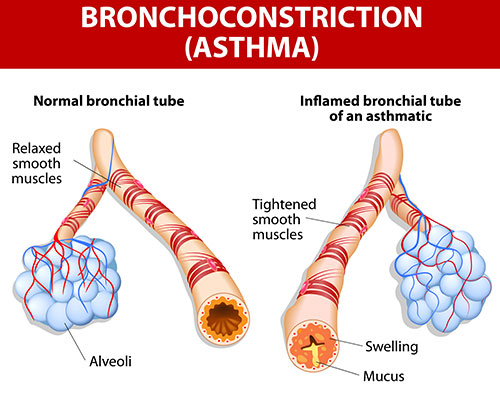
A person with asthma experiences inflammation of the bronchi, even when symptoms are not present. This causes a narrowing of the airways and an increased sensitivity to allergens or other stimuli. Exposure to these triggers often produces symptoms such as coughing, wheezing and an inability to breathe normally (shortness of breath).
Asthma primarily affects the bronchi, the large passageways that allow air to travel between the trachea (windpipe) and the lungs. The inner lining of these bronchial tubes is called the bronchial mucosa, and it houses two important contributors to asthma:
Mucous glands
These glands normally produce the proper amount of mucus to lubricate the airways. However, during an asthma attack they produce too much mucus, flooding and blocking the airways.
Inflammatory cells
These cells (including mast cells, lymphocytes and eosinophils) trigger inflammation in response to something the body perceives as a threat, such as allergens or irritants. The inflammation, in turn, allows for more blood to flow to the area, carrying cells to fight the threat. This is a natural system designed to protect body tissue, such as the lining of the bronchial tubes (mucosa). However, during an asthma attack, the tissues remain inflamed for extended periods of time.
During an asthma attack, exposure to an allergen or other stimuli (such as exercise or cold air) causes mast cells in the tissue of an asthmatic’s air passages to react by producing histamine, leukotrienes and other chemicals.
These chemicals cause the following chain reactions:
- The smooth muscle of the bronchi goes into bronchospasm and tightens, constricting the airways.
- The tissues lining the airways – which are often inflamed in asthmatics – become further inflamed, further narrowing the airways.
- The inflamed tissues produce excess mucus that fills and obstructs the airways.
Because airways are narrowed during an asthma attack, a person may experience chest tightness, coughing, wheezing and shortness of breath. In severe cases, where breathing becomes very difficult and low blood oxygen levels occur, asthma attacks can be fatal. About 5,000 deaths each year are attributed to asthma, according to the American Academy of Allergy, Asthma and Immunology (AAAAI).
Low blood oxygen levels can also be dangerous during pregnancy. Since a fetus depends on oxygen in the mother’s blood, uncontrolled asthma during pregnancy can lead to low birth weight and other complications.
Someone suffering through an asthma attack may appear to be gasping for breath. But in fact, it is easier to breathe in during an asthma attack than it is to breathe out. As more air flows in, it becomes trapped in the lungs, which become overinflated. Asthmatics continue to try to push this ever-increasing amount of inhaled air out of their lungs and through a narrowed airway, usually with limited success. Medications and other strategies are required to reverse the airway-narrowing process, allowing air to flow in and out of the body more easily.
According to the National Heart, Lung and Blood Institute, approximately 20 million people have been diagnosed with asthma, and 9 million of these patients are children. Asthma affects people of all ages. However, it often develops in childhood. The condition is more common in boys during childhood, but after puberty, more women have the condition.
Although asthma affects people of all races, African Americans are more likely to be hospitalized and die from the disease, when compared to Caucasians.
Types and differences of asthma
Asthma affects people in different ways and to various degrees.
There are four levels of severity used to classify different types of asthma:
- Mild intermittent. Symptoms appear up to two days a week and two nights a month.
- Mild persistent. Symptoms appear more than two nights a month and more than twice a week, but not more than once in a single day.
- Moderate persistent. Symptoms occur every day and more than one night a week.
- Severe persistent. Symptoms occur continuously throughout the day and frequently at night.
Asthma is most commonly triggered by allergens, such as dander, pollens, dust and molds. Known as allergic asthma, this form of asthma is found in approximately half of all asthma patients. But other stimuli also can trigger asthma symptoms or a full-blown asthma attack. Forms of asthma triggered by factors other than allergens include:
Exercise-induced asthma (EIA)
Asthma that occurs during vigorous physical activity. The condition usually manifests itself a few minutes after a person begins exercise. EIA afflicts a large percentage of asthmatics, and also can occur in individuals who usually have no other asthma symptoms.
NSAID-sensitive asthma
Severe asthma attacks that occur as a result of taking nonsteroidal anti-inflammatory drugs (NSAIDs), including aspirin and ibuprofen. People with this condition should consult a physician, who may recommend an alternative pain reliever, such as one that contains acetaminophen.
Nocturnal asthma
Asthma symptoms that manifest themselves primarily at night. It tends to occur between midnight and 8 a.m. and seems to be especially prevalent around 4 a.m.
Adult–onset asthma
Asthma that makes its first appearance in an adult after age 20. It is more common in women than in men.
Occupational asthma
Asthma that is triggered by conditions in the workplace. The main triggers for occupational asthma are airborne contaminants or allergens and extremes in temperature or humidity levels. It is most likely to occur among those who work with animals or animal–based products and in industries such as food service (especially bakery), chemicals, electronics, gardening, metalworking, painting, printing, plastics, rubber and textiles.
Potential causes of asthma
The source of asthma is not fully understood. Healthcare professionals believe a combination of genetic and environmental factors determine whether or not a person becomes asthmatic. The American Academy of Allergy, Asthma and Immunology estimates that 40 percent of children who have asthmatic parents will develop asthma.
One theory of asthma development involves immune system cells called T helper cells. It is known that T helper 2 cells (Th2) release chemicals that activate other cells known to contribute to inflammation. In a normally functioning immune system, this process is balanced by T helper 1 cells (Th1), which reduce inflammation. Evidence suggests that the T helper cells may be out of balance in asthmatics, preventing the body from controlling excess inflammation.
Immune system reactions are at the heart of another asthma theory, which states that the growing number of children with asthma stems from children having less exposure to certain types of bacteria, and infections than in the past. As a result, children have not developed the types of immune cells necessary to prevent asthma, according to this theory. Yet other research suggests that exposure to infections and allergens at an early age can increase the risk for developing asthma.
Physicians have noted that about 70 percent of people diagnosed as asthmatic also suffer from allergies. There also appears to be a strong association between a condition called sinusitis and asthma. Sinusitis, which is inflammation of the sinus cavities, occurs in 15 percent of people with asthma and 75 percent of those with severe asthma. By contrast, sinusitis occurs in about 5 percent of the general population.
This might occur because fluid from the sinuses may drain into the bronchial tubes, causing bronchitis. In turn, this might worsen asthma. It may also occur because the tissues in the sinuses and the airway linings are similar, so they may react to similar triggers.
In addition, all airway tissues are connected, and the inflammatory response may extend from the sinuses to the lower airways (bronchi).
Additional factors which may increase a person’s risk for asthma include:
- Living in the inner city, or another large urban area
- Exposure to secondhand smoke
- Exposure to occupational irritants, such a chemicals used in farming and hairdressing, and in the manufacturing of paint, steel, plastic and electronics
A person with asthma is more likely to experience symptoms or full–blown asthma attacks when exposed to certain allergens and stimuli, which are classified as asthma triggers. These include:
Allergens, such as:
- Pollen
- Mold
- Dust
- Cockroaches
- Pet dander
Irritants, such as:
- Air pollution
- Tobacco smoke
- Cold air
- Perfume
- Spray-on deodorants
- Strong odors from household chemicals, sprays or paints and other irritants
Other potential asthma triggers include:
- Certain foods
- Exercise
- Feathers in pillows
- Aspirin or ibuprofen
- Menstrual cycles (when hormonal changes may trigger asthma)
- Pregnancy
- Viral respiratory infections (including colds, bronchitis and flu)
- Stress
- Temperature changes
- Sinus infections
- Heartburn
- Sulfites (a preservative used in salad bars, dehydrated soups, alcohol and other foods)
- Gastroesophageal reflux disease (GERD)
Allergens are the most common trigger of asthma in those under the age of 30. Although allergens trigger the condition in many people over the age of 30, older adults tend to experience symptoms after exposure to irritants.
Physicians can help patients identify which factors trigger their asthma, and recommend steps the patients can take to avoid the triggers.
There also appears to be a link between obesity and asthma that is not yet understood. One study found that children who are obese at the time of puberty are three times more likely than their slimmer peers to continue to suffer from asthma into their teens. Other studies have found overweight school-age children are 50 percent more likely than those of normal weight to develop asthma, and those who had a high birthweight were 20 percent more likely to develop asthma later in childhood.
The association between asthma and obesity is also apparent in adults. Research has suggested that obese adults are three times more likely to develop asthma than thinner adults. There also appears to be a direct relationship between the amount of weight gained and the risk of developing asthma. Research suggests that an overweight person’s risk for asthma increases further as they gain more and more weight.
The mechanism behind the asthma-obesity link remains a mystery, though some research indicates that the two conditions share a gene that might link them together.
Signs and symptoms of asthma
Most experts now believe that asthma develops in an individual within the first few years of life. These symptoms sometimes can be observed during infancy, but there are other cases where asthma does not make its presence known until later in childhood or even into adulthood. Asthma symptoms are responsible for 1.8 million visits to the emergency room, making it one of the most common reasons for visits to emergency rooms and hospitalization.
The symptoms of asthma or an impending asthma attack are numerous.
They include:
- Rapid breathing
- Chest pain or tightness
- Chronic coughing
- Breathing difficulty
- Fever
- Headache
- Stuffy head
- Sneezing
- Scratchy or sore throat
- Itchy, watery eyes
- Runny nose
- Restlessness
- Listlessness
Some symptoms that appear to indicate asthma actually mask the presence of a separate condition, such as chronic obstructive pulmonary disease (COPD), gastroesophageal reflux disease (GERD) or sinusitis. Those who experience these symptoms should see a healthcare professional to obtain an accurate diagnosis.
It is important to note that the type and severity of symptoms experienced vary from person to person, as well as from episode to episode in the same person. The frequency of symptoms will also vary between patients. While some patients only experience symptoms every few months, others have symptoms every day. However, all patients can reduce the likelihood of asthma symptoms by consulting a physician and receiving proper treatment.
It is also important to note that signs and symptoms of asthma may vary in infants and children.
Diagnosis methods for asthma
A physician is likely to use several methods to determine whether or not a person has asthma. An individual’s medical history – including prior breathing problems, allergies or skin conditions – may offer important clues. A family history of asthma, eczema or allergies also may indicate an increased risk for asthma, as the condition appears to run in families with these conditions.
The physician may assess the severity of asthma using the following criteria:
- Extent to which asthma attacks interfere with normal activities
- Severity and duration of symptoms
- Degree of airway obstruction
Mild to moderate asthma is often characterized by tightness in the chest, coughing up mucus, difficulty sleeping and wheezing.
Severe attacks may be characterized by the following:
- Difficulty speaking
- Slight gray or bluish color to the lips and fingernail beds (cyanosis)
- Sucked-in appearance to the rib cage
- Breathlessness
Following the collection of a medical history, a physician will perform a physical examination to look for signs of asthma. The exam will focus on the respiratory tract, chest and skin. The physician will listen for wheezing and other sounds in the chest with a stethoscope (an instrument that uses rubber tubing that is placed in the ears and a cup-shaped device to detect sounds produced in the body). The physician will also use a nasal speculum (a handheld device with a telescope) to examine the inside of the nose for signs of allergies (e.g., swelling, polyps, increased secretions). The skin will be examined as well for signs of allergic conditions associated with asthma (e.g., eczema, hives).
Although, symptoms, a medical history and a physical exam can suggest the presence of asthma, diagnostic tests that measure an individual’s airflow are the primary means of uncovering asthma.
These and other tests may include:
Pulmonary function test
A test that measures how much air the lungs can hold and how quickly it is exhaled.
Bronchoprovocation test
A test that involves inducing a minor asthma attack to diagnose asthma when symptoms are not present. Most bronchoprovocation tests use histamine or methacholine but may include specific agents, such as food additives or environmental allergens.
Spirometry
A test that measures how much air a person blows out in a specific period of time, and how forcefully it is blown. It can reveal the extent of airway obstruction present, and how much of the obstruction is reversible.
Pulse oximetry
A test in which a probe is placed on a fingertip to measure the amount of oxygen in a person’s bloodstream.
Chest x-ray
An image of the chest produced using low doses of radiation. This test can be useful in detecting air trapped in the lungs. It may also be used to rule out other conditions and diseases known to cause symptoms similar to asthma.
Allergy skin test
A test used to identify a specific allergen that might be triggering asthma attacks. While allergies are a separate condition from asthma, allergic reactions often trigger attacks in asthmatics. During this test, a small amount of one or more allergens is introduced to the patient’s skin (through a prick, scratch, injection or patch). The skin is then examined for a positive reaction. A hive will usually indicate that an allergy to the substance is present. The test is not 100 percent accurate, but it can be an effective tool in diagnosing allergy triggers.
Patients can play a vital role in the ongoing diagnosis of their own asthma by using a peak flow meter. This device measures the amount of air flowing into and out of a patient’s lungs. By using it every day, patients can detect changes in their breathing capacity before the condition manifests itself in asthma symptoms. Peak flow meters can also help an individual determine the severity of an asthma attack once it has begun.
Other conditions may have similar symptoms, such as chronic obstructive pulmonary disease, emphysema, early onset of heart failure (cardiac asthma) and vocal cord dysfunction. A physician may perform other tests to rule out these conditions, including imaging tests and blood tests.
Treatment methods for asthma
Once an individual has been diagnosed with asthma, a physician will develop an asthma action plan to help the patient monitor the condition.
A typical plan will contain the following elements:
- A list of specific symptoms that often precede an individual’s asthma attacks
- Steps to take during an attack
- How to recognize a serious attack, and what to do about it
- How to recognize an emergency
- Changes in environment and behavior that can reduce the chances of an asthma flare–up
Current asthma treatment focuses primarily on preventing or reducing the inflammation process, and relaxing the smooth muscle that tightens during bronchospasm.
Healthcare professionals use asthma medications with two goals in mind:
- To keep the airway clear so the patient can breathe normally.
- To prevent airway remodeling, a thickening of the bronchial walls that can result from chronic inflammation and lead to permanent damage.
There are two categories of asthma medications:
Quick-relief medications
Also called “rescue” medications, these are designed to instantly relieve the symptoms of an asthma attack. They are usually not meant to be taken long–term.
Long-term-control medications
These are designed to minimize inflammation and prevent asthma flare-ups before they occur. Long-acting beta2 agonists are often used, as well as topical corticosteroids.
Patients with mild intermittent or mild persistent asthma may receive a quick-relief medication to aid them when their asthma flares-up. Those with moderate or severe asthma are more likely to need both quick-relief and long-term-control medications.
Asthma drugs can be delivered either in pill form or through an inhaler or nebulizer, which allows the drug to travel directly to the bronchial tubes while minimizing the effect on the rest of the body.
Bronchodilators are the primary class of medications used to treat asthma. These widen a person’s airways by relaxing the bronchial smooth muscle. Short-acting bronchodilators (such as beta2 agonists) provide immediate relief of asthma symptoms.
Long-acting bronchodilators (which include long-acting beta2 agonists) relieve symptoms for longer periods of time and are used once in the morning, and once at night.
It is important not to overuse these medications. Such abuse can make an asthmatic condition worse and possibly even increase the risk of death from asthma.
Other asthma medications stop an asthma attack before it starts by preventing the bronchial inflammation that constricts airways and hampers breathing.
These drugs include:
- Corticosteroids. Medications similar to the body’s own hormones. They prevent the inflammation associated with asthma attacks.
- Leukotriene modifiers. Medications that inhibit the role of leukotrienes, which are a type of chemical involved in an asthma attack. They may be taken daily or several times a day to prevent an asthma attack from occurring.
- Mast cell stabilizers. Medications that prevent mast cells from triggering reactions that can lead to an asthma attack or allergic reaction. This class of drug is rarely prescribed.
Medications
Prevention methods for asthma
Since it is not known why some people develop asthma and others do not, preventing the condition itself is not possible. However, there are several things that people can do to reduce the symptoms of asthma, including:
- Reducing exposure to environmental triggers, such as pollens, molds, secondhand tobacco smoke and animal dander.
- Leading a healthy lifestyle that includes proper rest, good nutrition and regular exercise.
- Taking all asthma medications as directed.
- Combating obesity. For reasons not fully understood, there appears to be a correlation between obesity and increased incidence of asthma. Obese individuals who lose weight often shed symptoms of asthma as well.
Gastroesophageal reflux disease (GERD) – a condition where stomach acid backs up into the esophagus – can trigger asthma symptoms, possibly as part of a nervous–system reflex. It is most likely to occur when an individual is lying down or sleeping after a big meal.
Steps to prevent GERD include:
- Refrain from snacking for two hours before bedtime
- Take antacids
- Avoid foods that trigger heartburn
- Raise the bed so the head is higher, forcing reflux downward
- Viral respiratory infections, such as colds or the flu, also can trigger asthma.
To minimize the likelihood of such symptoms:
- Obtain an annual flu shot
- Wash hands frequently
- Do not share glasses, utensils and other items with those who are sick
Long-term-control medications also can help prevent asthma attacks. In addition, there are certain breathing techniques that people with asthma can learn to can minimize the impact of asthma on breathing.
Certain forms of asthma, such as exercise-induced asthma, require specialized forms of prevention. Patients should discuss specific steps for symptom prevention with their physician.
Questions for your doctor about asthma
Preparing questions in advance can help patients to have more meaningful discussions with their physicians regarding their conditions. Patients may wish to ask their doctor the following questions related to asthma:
- Am I at risk for developing asthma?
- Are there steps I can take to prevent asthma?
- What symptoms may indicate that I have asthma?
- What tests will you use to determine if I have asthma?
- What may have caused me to develop asthma?
- What risks do I face by having asthma?
- What are my treatment options? How effective are they?
- Will I have to take medication for the rest of my life?
- Are there lifestyle modifications I should be making as the result of my diagnosis?
- How will the condition change as I get older?
- Are my children more likely to have asthma because I have the condition?
- George RB, Light RW, Matthay RA, Matthay MA. Asthma. In Chest Medicine: Essentials Of Pulmonary And Critical Care Medicine. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006.
- National Heart, Lung, and Blood Institute. Who Is At Risk For Asthma? 2014.
- The Medical Letter. Drugs Past Their Expiration Date. Med Lett Drugs Ther. 2009 Dec 14;51(1327):100-1.